|
Blog post by Marco Altini Heart rate variability (HRV) is a well-understood phenomenon allowing us to monitor objectively physiological stress. However, historically HRV analysis has been poorly standardized, leading to difficulties in properly designing and implementing studies as well as difficulties in comparing studies outcomes. The ease of access to HRV data today often obscures the complicated nature of understanding and correctly interpreting the information provided and underlying physiological processes. When designing HRV4Training we had to make several choices that I'd like to highlight here as transparency and clarity can only move this field forward. In this (updated) post we cover the basics of HRV and in particular the physiological mechanisms behind it, as well as best practices and a brief introduction to data analysis. I hope what follows can give some clarity to the ones interested in learning more about physiological stress and how their body responds to it. What is heart rate variability (HRV)?Each beat of our heart is triggered by an electrical impulse that can be easily recorded by an electrocardiogram (ECG), one of the most common ways to monitor heart activity. However, our heart doesn't beat at a constant frequency. When we talk about heart rate variability (HRV), we are interested in capturing the variability that occurs between heart beats. Let's look at 60 seconds of ECG data. This is some data I recorded on myself using the ECG Necklace, a research prototype we developed when I was working at imec, a few years ago. The device is a small sensor connected to 2 ECG leads: 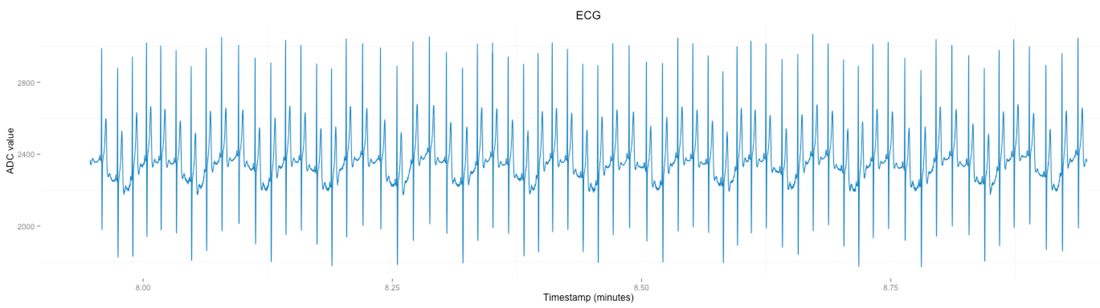 In technical jargon, the differences between beats are called RR intervals. The name derives from the fact that the shape of the ECG signal at each beat has been assigned letters (namely the QRS complex). For more on the QRS complex you can just have a quick look on the Wikipedia page, however the only relevant point here is that R represent the peak(s). Going back to my ECG, if we zoom in a bit and look at only 10 seconds, we can see clearly there are differences between intervals; some are shorter, other longer: 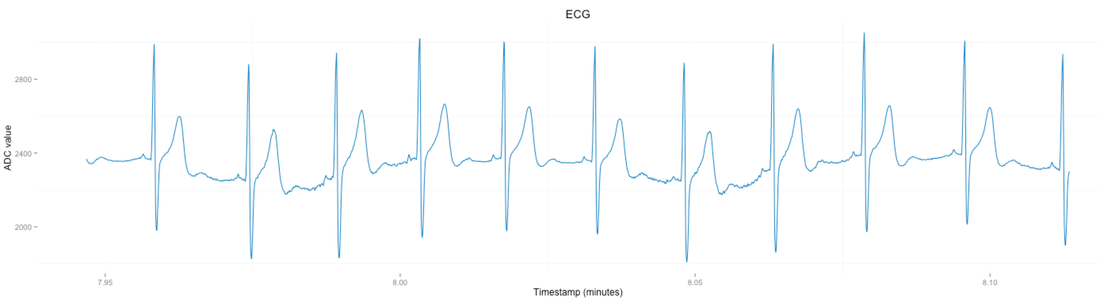 Another way we can look at these differences is by plotting an histogram of the RR intervals. Basically we stack up RR intervals that are of similar duration. This way it's actually much easier to see how the values are distributed over a rather wide range. For this plot, I used again the full minute of data from the first plot: 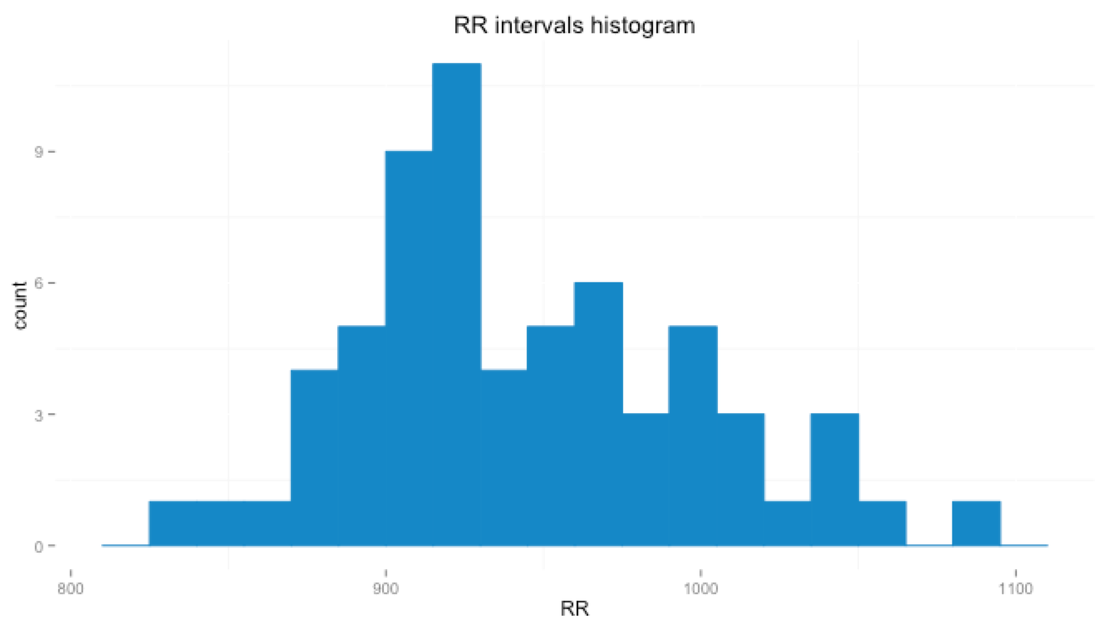 For this minute of data, RR interval values range between 832 and 1094 milliseconds. We can compute the instantaneous heart rate which gives us a range between 55 and 72 beats per minute. So far so good, now, why do we care about these differences in RR intervals? Why do we care?Physiological mechanisms mediating heart rhythmIn a nutshell, the human body senses stress through its senses and sends information to the brain, which determines how to deal with them. Sources of stress (stressors) are disruptions that trigger certain reactions as the body tries to maintain a state of balance, also called homeostasis, which is key to ensure optimal functioning. So what happens when we face a stressor? The central nervous system (CNS) is responsible for our visceral response to stimuli (Thayer et al.). Impulses from the brain and spinal cord to smooth muscles and (among others) the heart, are conducted by the autonomic nervous system (ANS), which is regulated by the hypothalamus. The autonomic nervous system (ANS) controls and regulates many functions of our body, from the heart beating to respiration. We typically think of the ANS in the context of its two branches, the sympathetic and parasympathetic nervous systems, that continuously regulate the ANS by acting in different directions. While the sympathetic nervous system is responsible for stimulating the body's fight or flight response, the parasympathetic nervous system is mainly responsible for the body's resting functions. HRV is mediated by neurons with parasympathetic and sympathetic origin and by the vagus nerve. Short term HRV, which is what is normally measured in consumer products, is mainly dominated by parasympathetic (vagal) influence. Measure of parasympathetic activity, controls many organs, including the heart, and connects processes like respiration and blood pressure to the heart. HRV can capture changes in the ANS non-invasively by quantifying one of the main controllers of the ANS, which is the vagus nerve, a cranial nerve which brings information from the body to the brain. Instead of measuring directly the vagus nerve or the amount of vagal influence on the heart - vagal tone, we measure processes that the vagus nerve alters, such as variability in heart beats. RecapLet's try to recap the whole physiological mechanism in a few words: as the body tries to maintain balance so that it can function optimally, heart rhythm is influenced by a series of processes going from the brain to the heart, processes that reflect the level of stress on the body. This is why HRV is such a powerful tool. How to use HRV is a complete different conversation to have, and highly dependent on the specific application (training or other), a hot topic these days. However - in my opinion - having insights on such physiological processes - can be eye opening even just as a tool for awareness. Best practices and other key practical pointsGet good dataBefore we can even start talking about interpreting data, we need to make sure we have collected valid measurements. This blog is full of posts in which we tried to analyze and compare different sensors (chest straps, wrist sensors, ear sensors, arm sensors, phone cameras, etc.) so that you can make informed decisions. If you use the app, we highly recommend using either the phone camera (validate here) or Polar sensors. 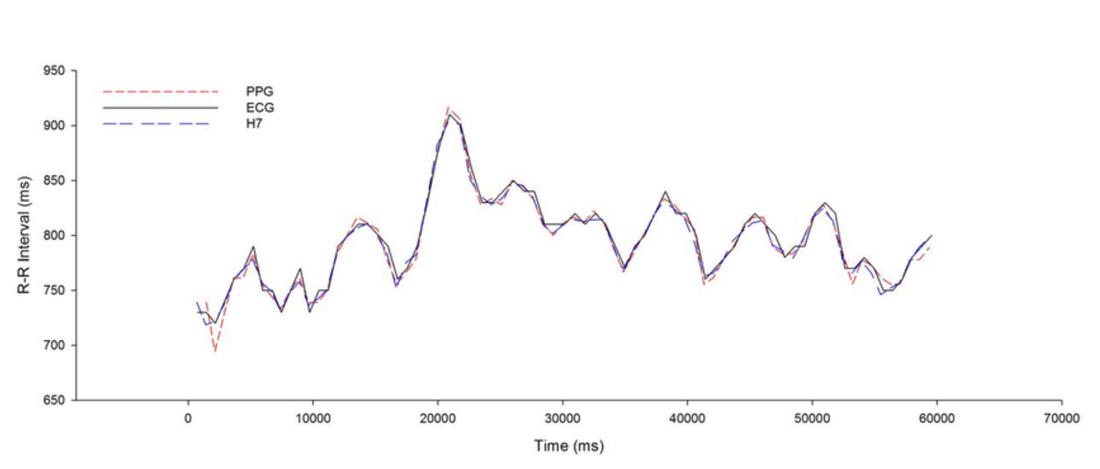 Simultaneous R-R interval of an individual subject during 60 seconds of recording for photoplethysmographic (PPG), Polar chest strap (H7) and electrocardiogram (ECG). Try to avoid confounding factors as much as possible (it's easy if you follow the best practices)The list of confounding factors for HRV analysis is pretty much endless. Why? Because as we explained at the beginning of this post, HRV is nothing less than a mechanism triggered by our body in response to stressors, and guess what, pretty much anything is a stressor. Quintana and Heathers provide great lists on their papers, but just to mention a few, nicotine, caffeine, time of the day, physical activity, alcohol intake, diet, digestion, water intake, age, etc. are all factors that can affect HRV measurements. How do we control for these factors? No need to despair, depending on the type of data we are collecting we have different methods to ensure we are not fooling ourselves by actually measuring the acute effect to some other random stressor that just affected us. In particular, as HRV4Training aims at quantifying overall physiological stress, and not the response of our system to a specific acute stressor (e.g. mental stress task, etc.), we can make the most of our measurements just by following a few best practices that aim at providing a clear, repeatable context for our measures. Best practicesBelow is a list and short description of a few steps that will ensure your morning measurement are valid, repeatable and meaningful over time.
What metric should you use?HRV is determined by computing so called features, starting from a series of RR intervals, or differences between heart beats. This means that on the contrary of heart rate, which can be thought of as an almost instantaneous value, HRV requires a certain amount of data to be accumulated, before it can be computed. Clinical practice recommends 5 minutes of data to be used for features extraction, however in the recent years more and more work was able to show that much shorter windows provide equivalence, and more practical 60 seconds recordings are sufficient [5], especially when we look at time domain features. Another important aspect to take into account is pre-processing to perform on RR intervals before we compute features. One of the most important steps is RR-Intervals correction, which prevents artifacts due to ectopic beats or motion from affecting features computation, as often reported in literature for HRV analysis. HRV4Training uses a configurable time window, so that you can go up to 5 minutes if you want to, but lets you also take shorter 60 seconds measurements. Additionally, RR interval correction is always performed after the recording, before computing features. We recommend using rMSSD as the main feature to look at (or Recovery Points, also derived from rMSSD) as a single metric which reflects very well parasympathetic activity and is not much affected by other confounding factors such as breathing. The vagus nerve acts on receptors signaling nodes to modulate pulse on a beat to beat basis while sympathetic activity has different pathways with slower signaling hence beat to beat changes computed as rMSSD reflect parasympathetic activity. Vagal influence has very short latency (less than 1s), while sympathetic influence is too slow to result in beat to beat differences (4-20s, see Nunan et al.). Another good feature is HF, however it suffers more from the influence of breathing frequency, hence we would recommend to stick to recovery points or rMSSD (rMSSD can be enabled in the app from Menu / Settings / HRV View / Advanced). More on this topic here. A note on artifactsHRV data is highly affected by artifacts, either in the measurement device (wrong beat detected, movement for PPG sensors), or in the actual data (ectopic beat, arrhythmias) that need to be handled properly. In HRV4Training we have different mechanisms (also highlighted in the paper above), that allow to correctly identify and remove artifacts. Check your app / device and ask what methods are used to deal with artifacts as even one single artifact can completely mess up your data, see for example below two consecutive minutes of data, the first one results in rMSSD = 79 ms while the second one - including one artifact - results in rMSSD = 201. 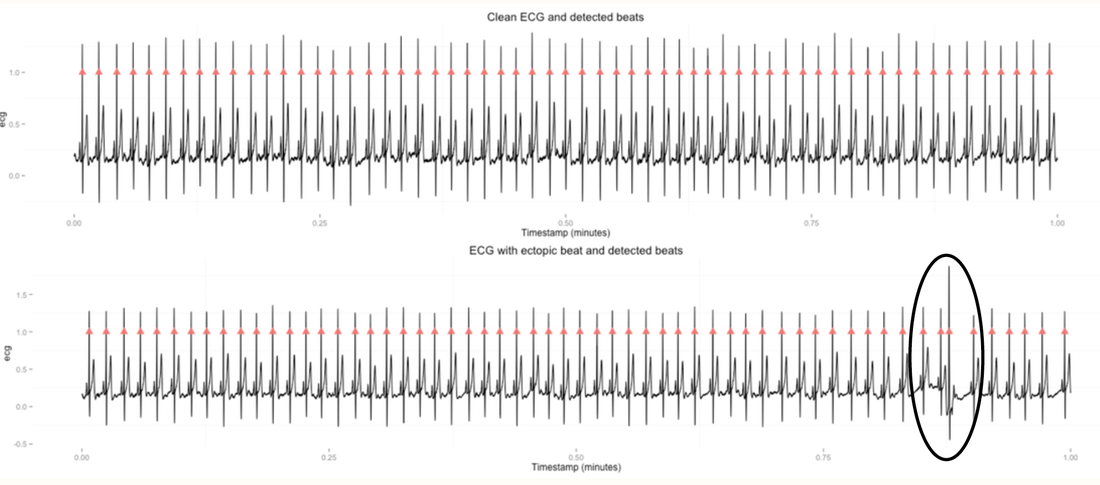 Artifact identification and removal: 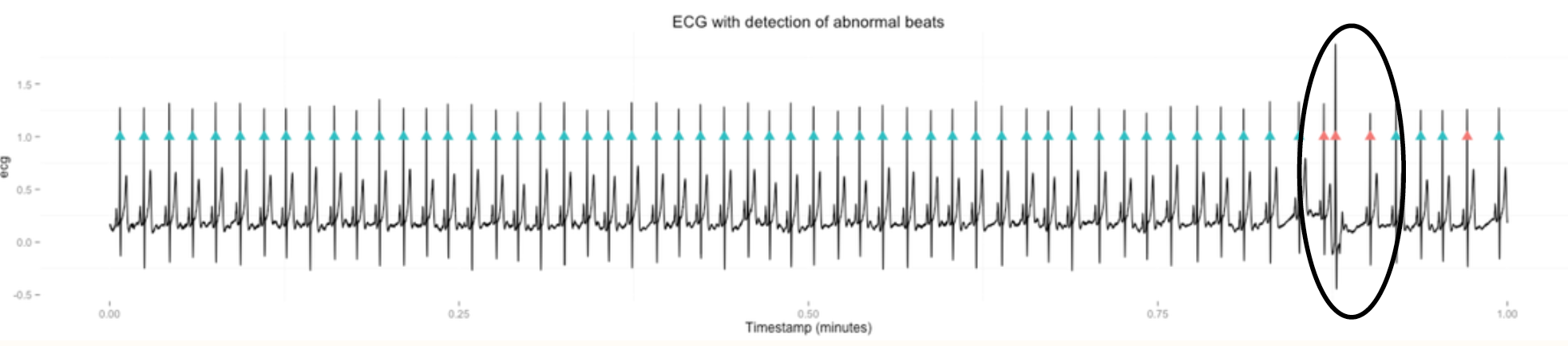 ECG recordings are the only ones that allow the researcher to see the QRS complex and hence the heart beats, leading to accurate identification of possible issues and meaningful correction. For mobile apps using either PPG or chest straps, there is no way to double check the data and make sure the identified beat is an artifact, even though usually a visual examination of the RR intervals timeseries can be sufficient. In certain cases (certain arrhythmias) it is simply not possible to compute meaningfully HRV. Measures repeatabilityIn general, there are always physiological variations as we are never in the same exact state, and just your mind wondering or swallowing can cause quite some differences, which is why the best practices above are so important. In general measuring HRV at random times during the day is not useful in the context of understanding overall physiological stress (it can still be valuable if we are trying to measure the response to a specific acute stressor). The inability of measurements taken at random times during the day to reflect underlying physiological stress was also shown recently by Mesquita et al., who showed that analyzing RMSSD from daily routine activities was not reliable, and therefore validity cannot be assumed as acute stressors during the day prevent reliability / repeatability. On the contrary, in standard conditions (morning measurements), and provided that you breathe normally and relax, back to back measurements should differ only by 5 to 20 ms in rMSSD (or less than 0.5 recovery points). The app is typically quite good at telling signal quality, and re-testing should not be necessary, as you might simply get more impatient and therefore affect the measurement. More on measures repeatability can be found here. Finally, the app deals with day to day variations and the fact that physiology is often changing by learning what variations are normal in your specific case, and building a model relying on the past 30 days of measurements so that only significant changes will be interpreted as such, when providing daily advice for your workouts. What to do with the dataAs explained above, the cardiovascular system is mostly controlled by autonomic regulation through the activity of sympathetic and parasympathetic pathways of the ANS and analysis of HRV permits analysis in this control mechanism [1]. Simply put, monitoring parasympathetic activity via HRV can provide insights on physiological stress, with higher level of stress resulting in lower HRV. In the context of sports, heavy training is responsible for shifting the cardiac autonomic balance toward a predominance of the sympathetic over the parasympathetic drive. This means that heavy training will reduce HRV and by monitoring HRV we can possibly optimize training, reduce the risk of overtraining and ultimately improve performance. On these last points, many research studies showed that short-term changes in HRV features, used to assess training load and recovery, are a reliable measure of parasympathetic activity [2, 3] and can even be user to guide training plans [4]. In one of our own publications we also highlighted how self reported training intensity was clearly correlated with physiological responses, across genders and age groups, in a sample of almost 800 users: 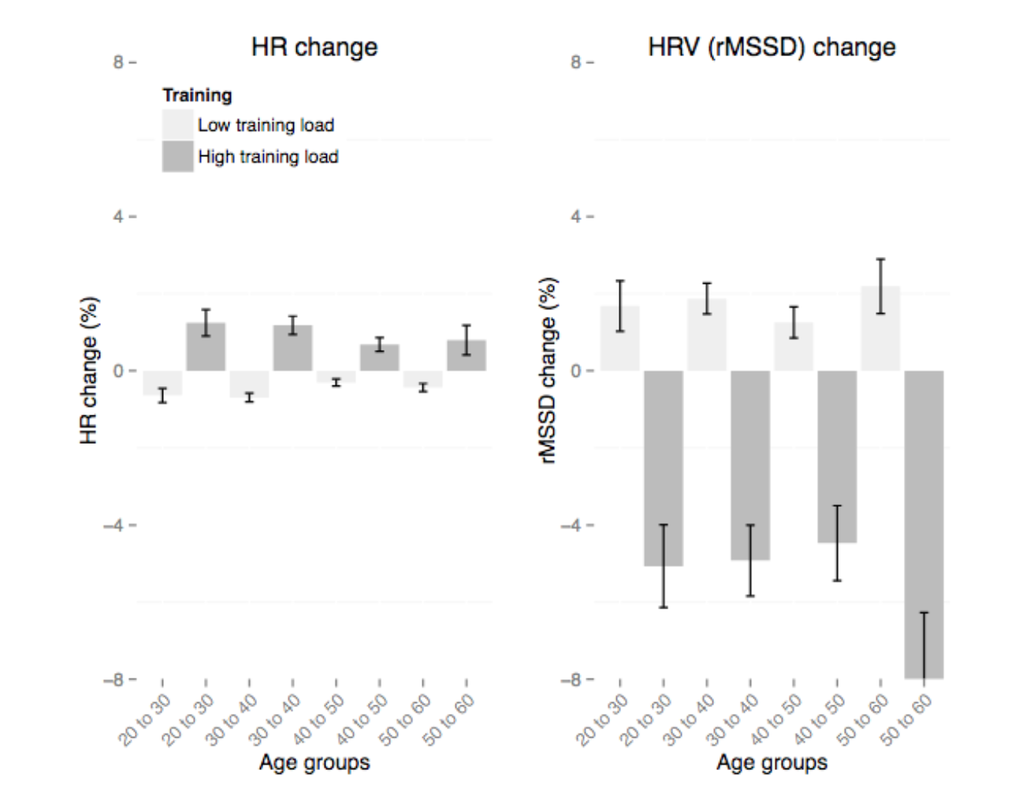 Relation between HR, HRV and training for different age groups. In all conditions HR is consistently increased on days following higher training load, while rMSSD is consistently decreased. The application to sports is the most widespread right now for a series of simple reasons: highly engaged users, 'easily' quantifiable stressor (training) - at least with respect to more challenging applications around mental health - as well as a faster feedback loop which drives engagement (performance, competition are in the weeks to months timeframe), with respect to other applications which might take years (e.g. aging or progression of a specific disease). In this post we won't go in depth on how to use HRV to guide training (what should you do if your HRV is normal? What if it is low? What if your baseline is trending down?, etc.), the point here is merely to highlight how training stressors can be easily captured in terms of the resulting physiological stress, as measured by HRV. For more on how to use HRV for your training, check out this blog post. Acute stressors: more than just trainingAnyone that used HRV4Training or other similar tools has probably learnt a little about how her/ his body responds to certain common stressors, for example day to day variations to acute stressors such as not only intense workouts but also getting sick, traveling, taking medication, alcohol intake etc. Below we can see a few examples (special thanks to Massi Milani for providing some of these): 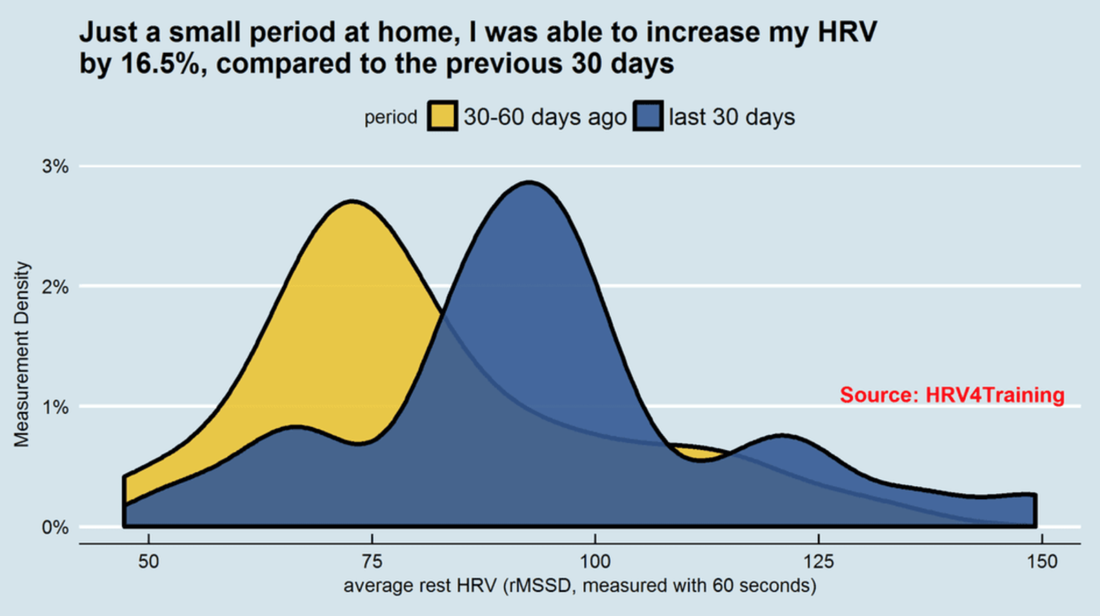 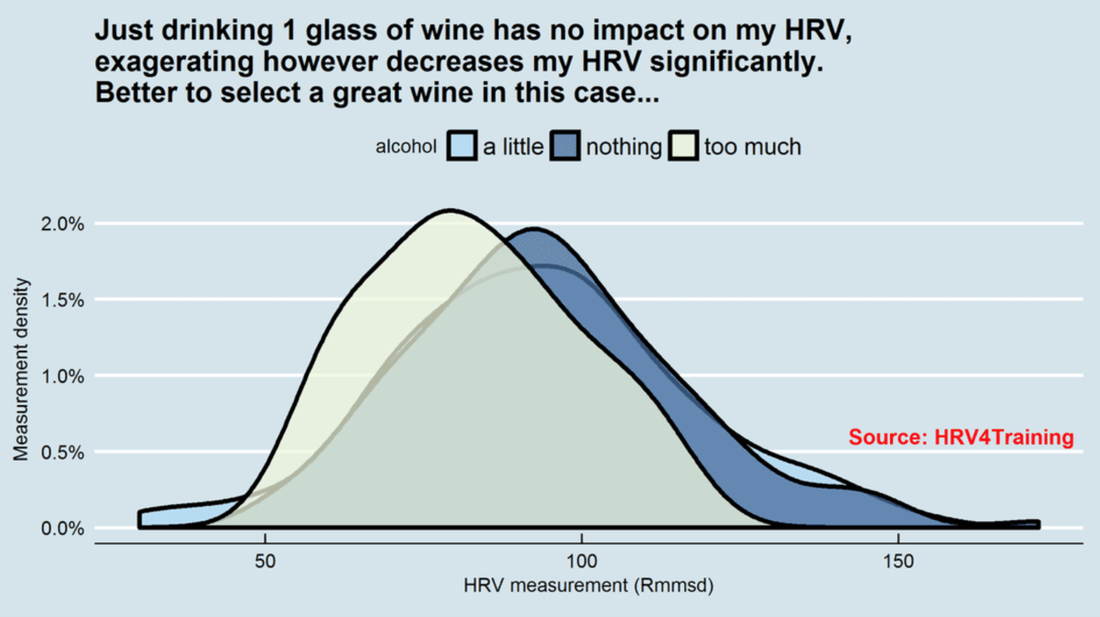 Below we have more than 1 million data points, from about 6000 people: 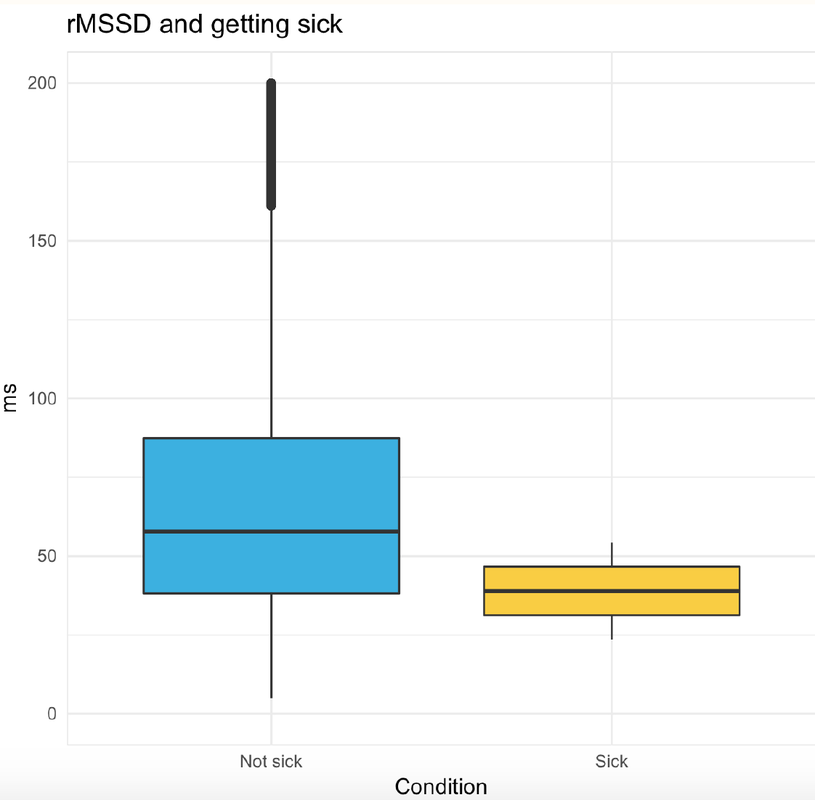 Acute stressors are typically quite strong, and can be detected even when analyzed in isolation as we’ve just seen. However, we should remember that all of the above factors (and many others) act simultaneously on the ANS (-> collect contextual data, which is why the morning Tags you fill in in HRV4Training are so important, physiological measurements per se are not that informative). Longitudinal data collectionLongitudinal data collection refers to collecting data for multiple days over time, which seems obvious to anyone here, but is far from being common in research. As technology has improved much in the past few years, measurements can finally be taken in optimal conditions (in terms of context and reductions of confounders, e.g. first thing in the morning). Much better than going to the lab every day. Additionally, compliancy increases as measuring requires less bulky technology / sensors (or no sensors at all). Collecting more data over time makes also data analysis more powerful, as we can understand much better what's normal for you, and provide meaningful advice based on a multitude of parameters and their evolution over time, instead of just sporadic spot checks, see for example our (experimental) HRV Trends analysis. Other examples of longitudinal data analysis are the progression of specific conditions, healthy ones (e.g. pregnancy) as well as disease (typical reduction in vagal tone, see diabetic neuropathy) as well as the adaptation to specific environments or activities, such as altitude adaptations (might be reflected in the degree of the reduction in HRV) or adaptations to training blocks. As pretty much anything affects the ANS, collecting longitudinal data representative of vagal tone can provide insights in many complex mechanisms taking place in health and disease. In the context of HRV analysis, we always stress the importance of looking at your own baseline and monitor deviations from the baseline. Our baseline HRV is probably affected by some factors that we cannot easily measure (genetics, for example, as reported once again recently), other factors that change but we have no control on (e.g. age), and factors we can probably influence (lifestyle). Hence, we highly recommend to focus only on relative changes, which is the most powerful way to make sense of your data, as shown in these articles: 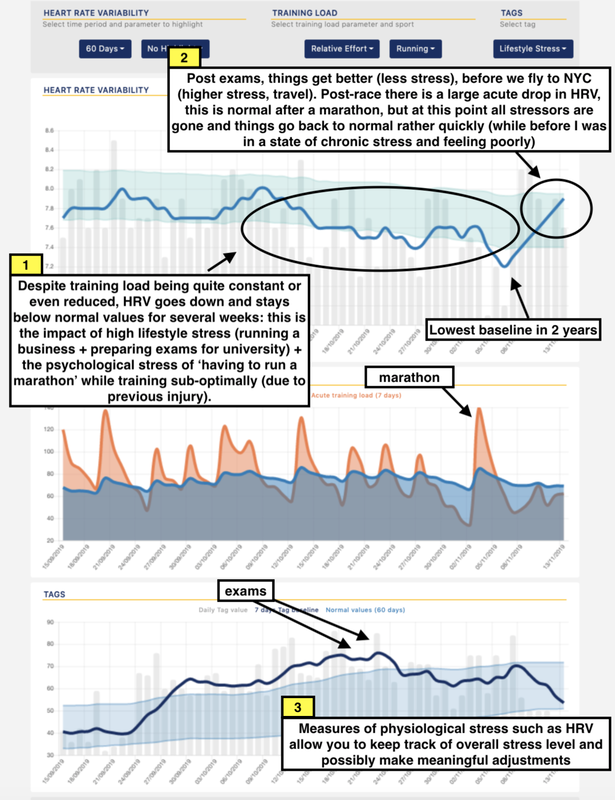 An example of how to use HRV data and analyze relative changes over time in response to training and lifestyle stressors. That's all for today, I hope the overview above is helpful in providing a decent understanding of the physiological processes that motivate the use of HRV and the many applications enabled by today's technologies. References[1] Aubert, André E., Bert Seps, and Frank Beckers. "Heart rate variability in athletes." Sports Medicine 33.12 (2003): 889-919.
[2] Garet, Martin, et al. "Individual interdependence between nocturnal ANS activity and performance in swimmers." Medicine and science in sports and exercise 36 (2004): 2112-2118. [3] Pichot, Vincent, et al. "Relation between heart rate variability and training load in middle-distance runners." Medicine and science in sports and exercise 32.10 (2000): 1729-1736. [4] Kiviniemi, Antti M., et al. "Endurance training guided individually by daily heart rate variability measurements." European journal of applied physiology 101.6 (2007): 743-751. [5] Esco, M. R., & Flatt, A. A. (2014). Ultra-Short-Term Heart Rate Variability Indexes at Rest and Post-Exercise in Athletes: Evaluating the Agreement with Accepted Recommendations. Journal of sports science & medicine, 13(3), 535. [6] HRV4Training: Large-Scale Longitudinal Training Load Analysis in Unconstrained Free-Living Settings Using a Smartphone Application. Available from: https://www.researchgate.net/publication/301998958_HRV4Training_Large-Scale_Longitudinal_Training_Load_Analysis_in_Unconstrained_Free-Living_Settings_Using_a_Smartphone_Application [accessed Nov 24 2017].
3 Comments
10/7/2015 08:55:01 am
Bravo well written with a limited amount of math that you really dont need to understand the HRV and its different aspects. ALso ( commented elsewhere ) You can tell you are a scientist with research background. While that is sometimes a detriment since scientists can be obtuse, in your case it is an asset. You clearly explained your product and in very easy to follow language. Well a few terms like sigma and mu could be put into english language. Well done. I just bought the polar and downloaded your app. I will let you know in a couple of weeks.
Marco Altini
10/7/2015 09:33:33 am
Thanks Russ!
Pierluigi Maini
5/14/2016 01:41:42 pm
Am in full agreement with the comments of my predecessor, rarely have seen a complex topic like this one being explained in such a simple and understandable way: Chapeau! Your comment will be posted after it is approved.
Leave a Reply. |


Register to the mailing list
and try the HRV4Training app! 
|